Digestion of Dietary Carbohydrates
Dietary carbohydrate from which humans gain energy enter the body in complex
forms, such as disaccharides and the polymers starch (amylose and amylopectin) and glycogen. The polymer cellulose is also consumed but not digested. The first step
in the metabolism of digestible carbohydrate is the conversion of the higher
polymers to simpler, soluble forms that can be transported across the intestinal
wall and delivered to the tissues. The breakdown of polymeric sugars begins in
the mouth. Saliva has a slightly acidic pH of 6.8 and contains lingual
amylase that begins the digestion of carbohydrates. The action of
lingual amylase is limited to the area of the mouth and the esophagus; it is
virtually inactivated by the much stronger acid pH of the stomach. Once the food
has arrived in the stomach, acid hydrolysis contributes to its degradation;
specific gastric proteases and lipases aid this process for proteins and fats,
respectively. The mixture of gastric secretions, saliva, and food, known
collectively as chyme, moves to the small
intestine.
The main polymeric-carbohydrate digesting enzyme of the small intestine is
a-amylase. This enzyme is secreted by the
pancreas and has the same activity as salivary amylase, producing disaccharides
and trisaccharides. The latter are converted to monosaccharides by intestinal
saccharidases, including maltases that hydrolyze di- and trisaccharides, and the
more specific disaccharidases, sucrase, lactase, and
trehalase. The net result is the almost complete conversion of
digestible carbohydrate to its constituent monosaccharides.
The resultant glucose and other simple carbohydrates are transported across
the intestinal wall to the hepatic portal vein and then to liver parenchymal
cells and other tissues. There they are converted to fatty acids, amino acids,
and glycogen, or else oxidized by the various catabolic pathways of cells.
Oxidation of glucose is known as glycolysis.Glucose is oxidized to either lactate or
pyruvate. Under aerobic conditions, the dominant product in most tissues is
pyruvate and the pathway is known as aerobic glycolysis. When oxygen is depleted, as for
instance during prolonged vigorous exercise, the dominant glycolytic product in
many tissues is lactate and the process is known
as anaerobic glycolysis.
back to the
top
The Energy Derived from Glucose Oxidation
Aerobic glycolysis of glucose to pyruvate, requires two equivalents of ATP
to activate the process, with the subsequent production of four equivalents of
ATP and two equivalents of NADH. Thus, conversion of one mole of glucose to two
moles of pyruvate is accompanied by the net production of two moles each of ATP
and NADH.
Glucose + 2 ADP + 2 NAD+ + 2
Pi -----> 2 Pyruvate + 2 ATP + 2 NADH + 2
H+
The NADH generated during glycolysis is used to fuel mitochondrial ATP
synthesis via oxidative
phosphorylation, producing either two or three equivalents of ATP depending
upon whether the glycerol
phosphate shuttle or the malate-aspartate
shuttle is used to transport the electrons from cytoplasmic NADH into the
mitochondria. The net yield from the oxidation of 1 mole of glucose to 2 moles
of pyruvate is, therefore, either 6 or 8 moles of ATP. Complete oxidation of the
2 moles of pyruvate, through the TCA cycle, yeilds
an additional 30 moles of ATP; the total yield, therefore being either 36 or 38
moles of ATP from the complete oxidation of 1 mole of glucose to CO2
and H2O.
back to the
top
The Individual Reactions of Glycolysis
The pathway of glycolysis can be seen as consisting of 2 separate phases.
The first is the chemical priming phase requiring energy in the form of ATP, and
the second is considered the energy-yielding phase. In the first phase, 2
equivalents of ATP are used to convert glucose to fructose 1,6-bisphosphate
(F1,6BP). In the second phase F1,6BP is degraded to pyruvate, with the
production of 4 equivalents of ATP and 2 equivalents of NADH.
 |
 |
| Pathway of glycolysis from glucose
to pyruvate. Substrates and products are in blue, enzymes are in green.
The two high energy intermediates whose oxidations are coupled to ATP
synthesis are shown in red (1,3-bisphosphoglycerate and
phosphoenolpyruvate). |
The Hexokinase Reaction
The ATP-dependent phosphorylation of glucose to form glucose 6-phosphate
(G6P)is the first reaction of glycolysis, and is catalyzed by tissue-specific
isoenzymes known as hexokinases. The phosphorylation accomplishes
two goals: First, the hexokinase reaction converts nonionic glucose into an
anion that is trapped in the cell, since cells lack transport systems for
phosphorylated sugars. Second, the otherwise biologically inert glucose becomes
activated into a labile form capable of being further metabolized.
Four mammalian isozymes of hexokinase are known (Types I - IV), with the
Type IV isozyme often referred to as glucokinase. Glucokinase is
the form of the enzyme found in hepatocytes. The high Km of
glucokinase for glucose means that this enzyme is saturated only at very high
concentrations of substrate.
 |
| Comparison of the activities of
hexokinase and glucokinase. The Km
for hexokinase is significantly lower (0.1mM) than that of
glucokinase (10mM). This difference ensures that non-hepatic
tissues (which contain hexokinase) rapidly and efficiently
trap blood glucose within their cells by converting it to
glucose-6-phosphate. One major function of the liver is to deliver glucose
to the blood and this in ensured by having a glucose phosphorylating
enzyme (glucokinase) whose Km for glucose is
sufficiently higher that the normal circulating concentration of glucose
(5mM). |
This feature of hepatic glucokinase allows the liver to buffer blood glucose. After meals, when postprandial blood
glucose levels are high, liver glucokinase is significantly active, which causes
the liver preferentially to trap and to store circulating glucose. When blood
glucose falls to very low levels, tissues such as liver and kidney---which
contain glucokinases but are not highly dependent on glucose---do not continue
to use the meager glucose supplies that remain available. At the same time,
tissues such as the brain, which are critically dependent on glucose, continue
to scavenge blood glucose using their low Km hexokinases, and as a
consequence their viability is protected. Under various conditions of glucose
deficiency, such as long periods between meals, the liver is stimulated to
supply the blood with glucose through the pathway of gluconeogenesis.
The levels of glucose produced during gluconeogenesis are insufficient to
activate glucokinase, allowing the glucose to pass out of hepatocytes and into
the blood.
The regulation of hexokinase and glucokinase activities is also different.
Hexokinases I, II, and III are allosterically inhibited by product (G6P)
accumulation, whereas glucokinases are not. The latter further insures liver
accumulation of glucose stores during times of glucose excess, while favoring
peripheral glucose utilization when glucose is required to supply energy to
peripheral tissues.
Phosphohexose Isomerase
The second reaction of glycolysis is an isomerization, in which G6P is
converted to fructose 6-phosphate (F6P). The enzyme catalyzing this reaction is
phosphohexose isomerase (also known as phosphoglucose
isomerase). The reaction is freely reversible at normal cellular
concentrations of the two hexose phosphates and thus catalyzes this
interconversion during glycolytic carbon flow and during gluconeogenesis.
6-Phosphofructo-1-Kinase (Phosphofructokinase-1,
PFK-1)
The next reaction of glycolysis involves the utilization of a second ATP to
convert F6P to fructose 1,6-bisphosphate (F1,6BP). This reaction is catalyzed by
6-phosphofructo-1-kinase, better known as
phosphofructokinase-1 or PFK-1. This reaction is not
readily reversible because of its large positive free energy (DG0' = +5.4 kcal/mol) in the reverse direction.
Nevertheless, fructose units readily flow in the reverse (gluconeogenic)
direction because of the ubiquitous presence of the hydrolytic enzyme,
fructose-1,6-bisphosphatase (F-1,6-BPase).
The presence of these two enzymes in the same cell compartment provides an
example of a metabolic futile cycle, which if unregulated would rapidly deplete
cell energy stores. However, the activity of these two enzymes is so highly
regulated that PFK-1 is considered to be the rate-limiting
enzyme of glycolysis and F-1,6-BPase is considered to be the rate-limiting enzyme in gluconeogenesis.
Aldolase
Aldolase catalyses the hydrolysis of F1,6BP into two 3-carbon products:
dihydroxyacetone phosphate (DHAP) and glyceraldehyde 3-phosphate (G3P). The
aldolase reaction proceeds readily in the reverse direction, being utilized for
both glycolysis and gluconeogenesis.
Triose Phosphate Isomerase The two
products of the aldolase reaction equilibrate readily in a reaction catalyzed by
triose phosphate isomerase. Succeeding reactions of glycolysis
utilize G3P as a substrate; thus, the aldolase reaction is pulled in the
glycolytic direction by mass action principals.
Glyceraldehyde-3-Phosphate
Dehydrogenase
The second phase of glucose catabolism features the energy-yielding
glycolytic reactions that produce ATP and NADH. In the first of these reactions,
glyceraldehyde-3-P dehydrogenase (G3PDH) catalyzes the
NAD+-dependent oxidation of G3P to 1,3-bisphosphoglycerate (1,3BPG)
and NADH. The G3PDH reaction is reversible, and the same enzyme catalyzes the
reverse reaction during gluconeogenesis.
Phosphoglycerate Kinase
The high-energy phosphate of 1,3-BPG is used to form ATP and
3-phosphoglycerate (3PG) by the enzyme phosphoglycerate kinase.
Note that this is the only reaction of glycolysis or gluconeogenesis that
involves ATP and yet is reversible under normal cell conditions. Associated with
the phosphoglycerate kinase pathway is an important reaction of erythrocytes,
the formation of 2,3BPG by the enzyme
bisphosphoglycerate mutase. 2,3BPG is an important regulator of hemoglobin's
affinity for oxygen. Note that 2,3-bisphosphoglycerate phosphatase
degrades 2,3BPG to 3-phosphoglycerate, a normal intermediate of glycolysis. The
2,3BPG shunt thus operates with the expenditure of 1 equivalent of ATP per
triose passed through the shunt. The process is not reversible under
physiological conditions.
Phosphoglycerate Mutase and Enolase
The remaining reactions of glycolysis are aimed at converting the relatively
low energy phosphoacyl-ester of 3PG to a high-energy form and harvesting the
phosphate as ATP. The 3PG is first converted to 2PG by phosphoglycerate
mutase and the 2PG conversion to phosphoenoylpyruvate (PEP) is catalyzed
by enolase
Pyruvate Kinase
The final reaction of aerobic glycolysis is catalyzed by the highly
regulated enzyme pyruvate kinase (PK). In this strongly exergonic
reaction, the high-energy phosphate of PEP is conserved as ATP. The loss of
phosphate by PEP leads to the production of pyruvate in an unstable enol form,
which spontaneously tautomerizes to the more stable, keto form of pyruvate. This
reaction contributes a large proportion of the free energy of hydrolysis of PEP.
back to the
top
Anaerobic Glycolysis
Under aerobic conditions, pyruvate in most cells is further metabolized via
the TCA cycle.
Under anaerobic conditions and in erythrocytes under aerobic conditions,
pyruvate is converted to lactate by the enzyme lactate dehydrogenase
(LDH), and the lactate is transported out of the cell into the circulation.
The conversion of pyruvate to lactate, under anaerobic conditions, provides the
cell with a mechanism for the oxidation of NADH (produced during the G3PDH
reaction) to NAD+; which occurs during the LDH catalyzed reaction.
This reduction is required since NAD+ is a necessary substrate for
G3PDH, without which glycolysis will cease. Normally, during aerobic glycolysis
the electrons of cytoplasmic NADH are transferred to mitochondrial carriers of
the oxidative
phosphorylation pathway generating a continuous pool of cytoplasmic
NAD+.
Aerobic glycolysis generates substantially more ATP per mole of glucose
oxidized than does anaerobic glycolysis. The utility of anaerobic glycolysis to
a muscle cell when it needs large amounts of energy stems from the fact that the
rate of ATP production from glycolysis is approximately 100X faster than from
oxidative phosphorylation. During exertion muscle cells do not need to energize
anabolic reaction pathways. The requirement is to generate the maximum amount of
ATP, for muscle contraction, in the shortest time frame. This is why muscle
cells derive almost all of the ATP consumed during exertion from anaerobic
glycolysis.
back to the
top
Regulation of Glycolysis
The reactions catalyzed by hexokinase, PFK-1 and PK all proceed with a
relatively large free energy decrease. These nonequilibrium reactions of
glycolysis would be ideal candidates for regulation of the flux through
glycolysis. Indeed, in vitro studies have shown all three enzymes to be
allosterically controlled.
Regulation of hexokinase, however, is not the major control point in
glycolysis. This is due to the fact that large amounts of G6P are derived from
the breakdown of glycogen (the predominant mechanism of carbohydrate entry into
glycolysis in skeletal muscle) and, therefore, the hexokinase reaction is not
necessary. Regulation of PK is important for reversing glycolysis when ATP is
high in order to activate gluconeogenesis. As such this enzyme catalyzed
reaction is not a major control point in glycolysis. The rate limiting step in
glycolysis is the reaction catalyzed by PFK-1.
PFK-1 is a tetrameric enzyme that exist in two conformational states termed
R and T that are in equilibrium. ATP is both a substrate and an allosteric
inhibitor of PFK-1. Each subunit has two ATP binding sites, a substrate site and
an inhibitor site. The substrate site binds ATP equally well when the tetramer
is in either conformation. The inhibitor site binds ATP essentially only when
the enzyme is in the T state. F6P is the other substrate for PFK-1 and it also
binds preferentially to the R state enzyme. At high concentrations of ATP, the
inhibitor site becomes occupied and shifting the equilibrium of PFK-1
comformation to that of the T state decreasing PFK-1's ability to bind F6P. The
inhibition of PFK-1 by ATP is overcome by AMP which binds to the R state of the
enzyme and, therefore, stabilizes the conformation of the enzyme capable of
binding F6P. The most important allosteric regulator of both glycolysis and
gluconeogenesis is fructose 2,6-bisphosphate,
F2,6BP, which is not an intermediate in glycolysis or in
gluconeogenesis.
 |
| Regulation of glycolysis and
gluconeogenesis by fructose 2,6-bisphosphate
(F2,6BP). The major sites for regulation of glycolysis and
gluconeogenesis are the phosphofructokinase-1 (PFK-1) and
fructose-1,6-bisphosphatase (F-1,6-BPase) catalyzed
reactions. PFK-2 is the kinase activity and F-2,6-BPase is the phosphatase
activity of the bi-functional regulatory enzyme,
phosphofructokinase-2/fructose-2,6-bisphosphatase. PKA is cAMP-dependent
protein kinase which phosphorylates PFK-2/F-2,6-BPase turning on the
phosphatase activity. (+ve) and (-ve) refer to positive and negative
activities, respectively. |
The synthesis of F2,6BP is catalyzed by the bifunctional enzyme
phosphofructokinase-2/fructose-2,6-bisphosphatase
(PFK-2/F-2,6-BPase). In the nonphosphorylated form the enzyme is known as
PFK-2 and serves to catalyze the synthesis of F2,6BP by phosphorylating fructose
6-phosphate. The result is that the activity of PFK-1 is greatly stimulated and
the activity of F-1,6-BPase is greatly inhibited.
Under conditions where PFK-2 is active, fructose flow through the
PFK-1/F-1,6-BPase reactions takes place in the glycolytic direction, with a net
production of F1,6BP. When the bifunctional enzyme is phosphorylated it no
longer exhibits kinase activity, but a new active site hydrolyzes F2,6BP to F6P
and inorganic phosphate. The metabolic result of the phosphorylation of the
bifunctional enzyme is that allosteric stimulation of PFK-1 ceases, allosteric
inhibition of F-1,6-BPase is eliminated, and net flow of fructose through these
two enzymes is gluconeogenic, producing F6P and eventually glucose.
The interconversion of the bifunctional enzyme is catalyzed by cAMP-dependent protein
kinase (PKA), which in turn is regulated by circulating peptide hormones.
When blood glucose levels drop, pancreatic insulin production falls, glucagon
secretion is stimulated, and circulating glucagon is highly increased. Hormones
such as glucagon bind to plasma membrane receptors on liver cells, activating
membrane-localized adenylate cyclase leading to an increase in the
conversion of ATP to cAMP. cAMP binds to the regulatory subunits of PKA, leading
to release and activation of the catalytic subunits. PKA phosphorylates numerous
enzymes, including the bifunctional PFK-2/F-2,6-BPase. Under these conditions
the liver stops consuming glucose and becomes metabolically gluconeogenic,
producing glucose to reestablish normoglycemia.
Regulation of glycolysis also occurs at the step catalyzed by pyruvate
kinase, (PK). The liver enzyme has been most studied in vitro.
This enzyme is inhibited by ATP and acetyl-CoA and is activated by F1,6BP. The
inhibition of PK by ATP is similar to the effect of ATP on PFK-1. The binding of
ATP to the inhibitor site reduces its affinity for PEP. The liver enzyme is also
controlled at the level of synthesis. Increased carbohydrate ingestion induces
the synthesis of PK resulting in elevated cellular levels of the enzyme.
A number of PK isozymes have been described. The liver isozyme (L-type),
characteristic of a gluconeogenic tissue, is regulated via phosphorylation by
PKA, whereas the M-type isozyme found in brain, muscle, and other glucose
requiring tissue is unaffected by PKA. As a consequence of these differences,
blood glucose levels and associated hormones can regulate the balance of liver
gluconeogenesis and glycolysis while muscle metabolism remains unaffected.
In erythrocytes, the fetal PK isozyme has much greater activity than the
adult isozyme; as a result, fetal erythrocytes have comparatively low
concentrations of glycolytic intermediates. Because of the low steady-state
concentration of fetal 1,3BPG, the 2,3BPG shunt is
greatly reduced in fetal cells and little 2,3BPG is formed. Since 2,3BPG is a
negative effector of hemoglobin affinity for oxygen, fetal erythrocytes have a
higher oxygen affinity than maternal erythrocytes. Therefore, transfer of oxygen
from maternal hemoglobin to fetal hemoglobin is favored, assuring the fetal
oxygen supply. In the newborn, an erythrocyte isozyme of the M-type with
comparatively low PK activity displaces the fetal type, resulting in an
accumulation of glycolytic intermediates. The increased 1,3BPG levels activate
the 2,3BPG shunt, producing 2,3BPG needed to regulate oxygen binding to
hemoglobin.
Genetic diseases of adult erythrocyte PK are known in which the kinase is
virtually inactive. The erythrocytes of affected individuals have a greatly
reduced capacity to make ATP and thus do not have sufficient ATP to perform
activities such as ion pumping and maintaining osmotic balance. These
erythrocytes have a short half-life, lyse readily, and are responsible for some
cases of hereditary hemolytic anemia.
The liver PK isozyme is regulated by phosphorylation, allosteric effectors,
and modulation of gene expression. The major allosteric effectors are F1,6BP,
which stimulates PK activity by decreasing its Km(app) for PEP, and
for the negative effector, ATP. Expression of the liver PK gene is strongly
influenced by the quantity of carbohydrate in the diet, with high-carbohydrate
diets inducing up to 10-fold increases in PK concentration as compared to low
carbohydrate diets. Liver PK is phosphorylated and inhibited by PKA, and thus it
is under hormonal control similar to that described earlier for PFK-2.
Muscle PK (M-type) is not regulated by the same mechanisms as the liver
enzyme. Extracellular conditions that lead to the phosphorylation and inhibition
of liver PK, such as low blood glucose and high levels of circulating glucagon,
do not inhibit the muscle enzyme. The result of this differential regulation is
that hormones such as glucagon and epinephrine favor liver gluconeogenesis by
inhibiting liver glycolysis, while at the same time, muscle glycolysis can
proceed in accord with needs directed by intracellular conditions.
back to the
top
Metabolic Fates of Pyruvate
Pyruvate is the branch point molecule of glycolysis. The ultimate fate of
pyruvate depends on the oxidation state of the cell. In the reaction catalyzed
by G3PDH a molecule of NAD+ is reduced to NADH. In order to maintain
the re-dox state of the cell, this NADH must be re-oxidized to NAD+.
During aerobic glycolysis this occurs in the mitochondrial electron transport
chain generating ATP. Thus, during aerobic glycolysis ATP is generated from
oxidation of glucose directly at the PGK and PK reactions as well as indirectly
by re-oxidation of NADH in the oxidative
phosphorylation pathway. Additional NADH molecules are generated during the
complete aerobic oxidation of pyruvate in the TCA cycle.
Pyruvate enters the TCA cycle in the form of acetyl-CoA which is the product of the pyruvate
dehydrogenase reaction. The fate of pyruvate during anaerobic glycolysis
is reduction to lactate.
back to the
top
Lactate Metabolism
During anaerobic glycolysis, that period of time when glycolysis is
proceeding at a high rate (or in anaerobic organisms), the oxidation of NADH
occurs through the reduction of an organic substrate. Erythrocytes and skeletal
muscle (under conditions of exertion) derive all of their ATP needs through
anaerobic glycolysis. The large quantity of NADH produced is oxidized by
reducing pyruvate to lactate. This reaction is carried out by lactate
dehydrogenase, (LDH). The lactate produced during anaerobic glycolysis
diffuses from the tissues and is transproted to highly aerobic tissues such as
cardiac muscle and liver. The lactate is then oxidized to pyruvate in these
cells by LDH and the pyruvate is further oxidized in the TCA cycle. If the
energy level in these cells is high the carbons of pyruvate will be diverted
back to glucose via the gluconeogenesis pathway.
Mammalian cells contain two distinct types of LDH subunits, termed M and H.
Combinations of these different subunits generates LDH isozymes with different
characteristics. The H type subunit predominates in aerobic tissues such as
heart muscle (as the H4 tetramer) while the M subunit predominates in anaerobic
tissues such as skeletal muscle as the M4 tetramer). H4 LDH has a low
Km for pyruvate and also is inhibited by high levels of pyruvate. The
M4 LDH enzyme has a high Km for pyruvate and is not inhibited by
pyruvate. This suggsts that the H-type LDH is utilized for oxidizing lactate to
pyruvate and the M-type the reverse.
back to the
top
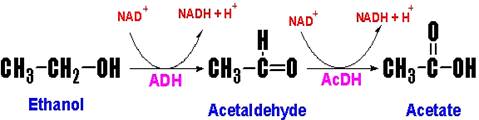
Ethanol Metabolism
Animal cells (primarily hepatocytes) contain the cytosolic enzyme
alcohol dehydrogenase (ADH) which oxidizes ethanol to
acetaldehyde. Acetaldehyde then enters the mitochondria where it is oxidized to
acetate by acetaldehyde dehydrogenase (AcDH).
 |
Acetaldehyde forms adducts with proteins, nucleic acids and other compounds,
the results of which are the toxic side effects (the hangover) that are associated with alcohol consumption. The
ADH and AcDH catalyzed reactions also leads to the reduction of NAD+
to NADH. The metabolic effects of ethanol intoxication stem from the actions of
ADH and AcDH and the resultant cellular imbalance in the NADH/NAD+.
The NADH produced in the cytosol by ADH must be reduced back to NAD+
via either the malate-aspartate
shuttle or the glycerol-phosphate
shuttle. Thus, the ability of an individual to metabolize ethanol is
dependent upon the capacity of hepatocytes to carry out eother of these 2
shuttles, which in turn is affected by the rate of the TCA cycle in the
mitochondria whose rate of function is being impacted by the NADH produced by
the AcDH reaction. The reduction in NAD+ impairs the flux of glucose
through glycolysis at the glyceraldehyde-3-phosphate dehydrogenase
reaction, thereby limiting energy production. Additionally, there is an
increased rate of hepatic lactate production due to the effect of increased NADH
on direction of the hepatic lactate dehydrogenase (LDH) reaction.
This reverseral of the LDH reaction in hepatocytes diverts pyruvate from
gluconeogenesis leading to a reduction in the capacity of the liver to deliver
glucose to the blood.
In addition to the negative effects of the altered NADH/NAD+
ratio on hepatic gluconeogenesis, fatty acid oxidation is also reduced as this
process requires NAD+ as a cofactor. In fact the opposite is true,
fatty acid synthesis is increased and there is an increase in triacylglyceride
production by the liver. In the mitocondria, the production of acetate from
acetaldehyde leads to increased levels of acetyl-CoA. Since the increased
generation of NADH also reduces the activity of the TCA cycle, the acetyl-CoA is
diverted to fatty acid synthesis. The reduction in cytosolic NAD+
leads to reduced activity of glycerol-3-phosphate dehydrogenase
(in the glcerol 3-phosphate to DHAP direction) resulting in increased levels of
glycerol 3-phosphate which is the backbone for the synthesis of the
triacylglycerides. Both of these two events lead to fatty acid deposition in the
liver leading to fatty liver syndrome.
back to the
top
Regulation of Blood Glucose Levels
If for no other reason, it is because of the demands of the brain for
oxidizable glucose that the human body exquisitely regulates the level of
glucose circulating in the blood. This level is maintained in the range of 5mM.
Nearly all carbohydrates ingested in the diet are converted to glucose
following transport to the liver. Catabolism of dietary or cellular proteins
generates carbon atoms that can be utilized for glucose synthesis via gluconeogenesis.
Additionally, other tissues besides the liver that incompletely oxidize glucose
(predominantly skeletal muscle and erythrocytes) provide lactate that can be
converted to glucose via gluconeogenesis.
Maintenance of blood glucose homeostasis is of paramount importance to the
survival of the human organism. The predominant tissue responding to signals
that indicate reduced or elevated blood glucose levels is the liver. Indeed, one
of the most important functions of the liver is to produce glucose for the
circulation. Both elevated and reduced levels of blood glucose trigger hormonal
responses to initiate pathways designed to restore glucose homeostasis. Low
blood glucose triggers release of glucagon from
pancreatic a-cells. High blood glucose triggers release
of insulin from pancreatic b-cells. Additional signals, ACTH and
growth hormone, released from the pituitary act to increase blood
glucose by inhibiting uptake by extrahepatic tissues. Glucocorticoids also act to increase blood glucose levels
by inhibiting glucose uptake. Cortisol, the major
glucocorticoid released from the adrenal cortex, is secreted in response to the
increase in circulating ACTH. The adrenal medullary hormone, epinephrine, stimulates production of glucose by activating
glycogenolysis in response to stressful stimuli.
Glucagon binding to its' receptors on the surface of liver cells triggers an
increase in cAMP production leading to an increased rate of glycogenolysis
by activating glycogen phosphorylase via the PKA-mediated
cascade. This is the same response hepatocytes have to epinephrine release.
The resultant increased levels of G6P in hepatocytes is hydrolyzed to free
glucose, by glucose-6-phosphatase, which then diffuses to the
blood. The glucose enters extrahepatic cells where it is re-phosphorylated by
hexokinase. Since muscle and brain cells lack
glucose-6-phosphatase, the glucose-6-phosphate product of
hexokinase is retained and oxidized by these tissues.
In opposition to the cellular responses to glucagon (and epinephrine on
hepatocytes), insulin stimulates extrahepatic uptake of glucose from the blood
and inhibits glycogenolysis in extrahepatic cells and conversely stimulates
glycogen synthesis. As the glucose enters hepatocytes it binds to and inhibits
glycogen phosphorylase activity. The binding of free glucose
stimulates the de-phosphorylation of phosphorylase thereby,
inactivating it. Why is it that the glucose that enters hepatocytes is not
immediately phosphorylated and oxidized? Liver cells contain an isoform of
hexokinase called glucokinase. Glucokinase has a much lower
affinity for glucose than does hexokinase. Therefore, it is not fully active at
the physiological ranges of blood glucose. Additionally, glucokinase is not
inhibited by its product G6P, whereas, hexokinase is inhibited by G6P.
One major response of non-hepatic tissues to insulin is the recruitment, to
the cell surface, of glucose transporter complexes. Glucose transporters
comprise a family of five members, GLUT-1 to
GLUT-5. GLUT-1 is ubiquitously distributed in various tissues. GLUT-2
is found primarily in intestine, kidney and liver. GLUT-3 is also found in the
intestine and GLUT-5 in the brain and testis. Insulin-sensitive tissues such as
skeletal muscle and adipose tissue contain GLUT-4. When the concentration of
blood glucose increases in response to food intake, pancreatic GLUT-2 molecules
mediate an increase in glucose uptake which leads to increased insulin
secretion.
Hepatocytes, unlike most other cells, are freely permeable to glucose and
are, therefore, essentially unaffected by the action of insulin at the level of
increased glucose uptake. When blood glucose levels are low the liver does not
compete with other tissues for glucose since the extrahepatic uptake of glucose
is stimulated in response to insulin. Conversely, when blood glucose levels are
high extrahepatic needs are satisfied and the liver takes up glucose for
conversion into glycogen for
future needs. Under conditions of high blood glucose, liver glucose levels will
be high and the activity of glucokinase will be elevated. The G6P produced by
glucokinase is rapidly converted to G1P by phosphoglucomutase,
where it can then be incorporated into glycogen.
back
to the top
Back to Topics<<<<
This article has been modified by Dr. M. Javed Abbas.
If you have any comments please do not hesitate to sign my Guest Book.
20:38 21/12/2002
|